Kidney Disease Replacement Therapy
When kidney disease progresses to end-stage renal failure (loss of 85-90% kidney function) and is accompanied by uremic symptoms, kidney replacement therapy becomes necessary. This therapy includes dialysis (hemodialysis, peritoneal dialysis), kidney transplantation, and palliative care.Dialysis acts as a substitute for healthy kidneys, maintaining your body's functions.
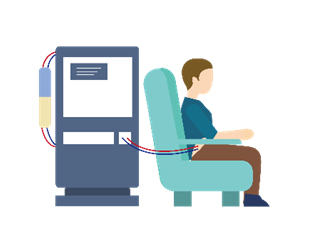
Hemodialysis: Commonly referred to as "kidney dialysis," it involves using a hemodialysis machine and an artificial kidney (dialyzer) to filter waste and excess fluids from the blood. Generally, individuals require 2-3 sessions per week at a dialysis center, with each session lasting around 4-5 hours. A functioning vascular access is essential for hemodialysis, and this access needs to be prepared prior to starting the treatment.

Peritoneal Dialysis: Peritoneal dialysis involves infusing dialysis solution into the abdominal cavity through a catheter. Using osmotic pressure, this method clears waste and excess fluids from the body. Patients can perform exchanges of the dialysis solution at home. There are two types: Continuous Ambulatory Peritoneal Dialysis (CAPD), where fluid exchanges are done 4-5 times a day, and Automated Peritoneal Dialysis (APD), which involves automated exchanges during sleep for about 8 hours. A surgical procedure is required to implant the catheter before starting peritoneal dialysis.
Kidney Transplantation: A healthy kidney is transplanted into the patient's lower abdomen on either the left or right side. A successful transplant can replace the failed kidney and restore kidney function. However, long-term use of immunosuppressant drugs and regular monitoring is necessary. In Taiwan, kidney donors can be fifth-degree relatives or organ donors from brain-dead patients. Tissue matching is essential before transplantation can occur.
Palliative Care: Palliative care is considered when factors such as age, daily functioning, the nature of underlying diseases (e.g., terminal cancer, prolonged ventilator use, or organ failure), or when continuing dialysis wouldn't improve the quality of life. This involves either discontinuing or reducing dialysis frequency (e.g., 2 or 1 session per week) to provide comfort-focused care and symptom relief, while addressing individual needs.
